
Victory Friday | Issue 137
Orthopedic Insights: Breathing & Orthopedics, Part I • Side Lunge Soleus Raise • The Other Ankle Mobility • Cross-Training Culprit in Chronic Pain?

“You can’t wish for both growth and comfort. The price of the first is the second.”
~ Alex Hormozi
Victory Friday is a weekly digest of reflections, insights, and tools from the world of functional manual and performance medicine. It is a free weekly publication. To support Victory Friday with a paid subscription, click below:
Happy Friday! Late-spring pollen blooms might conspire against you, but we begin a two-part series this week on how breathing moves our whole body! Then, an overlooked but crucial “reverse” stretch can unlock a stubborn ankle, followed by an unconventional way to work lower leg strength and balance. Finally: when cross-training keeps you injured! Check it out!
What I’m Into: Breathing & Orthopedics, Part I. I once again find myself exploring the implications of breathing on our orthopedic system.
Breathing is the most consistent, largest-magnitude movement in the body.
Whether we are active or asleep, it is a “movement” we perform 12-20+ times per minute, around the clock.
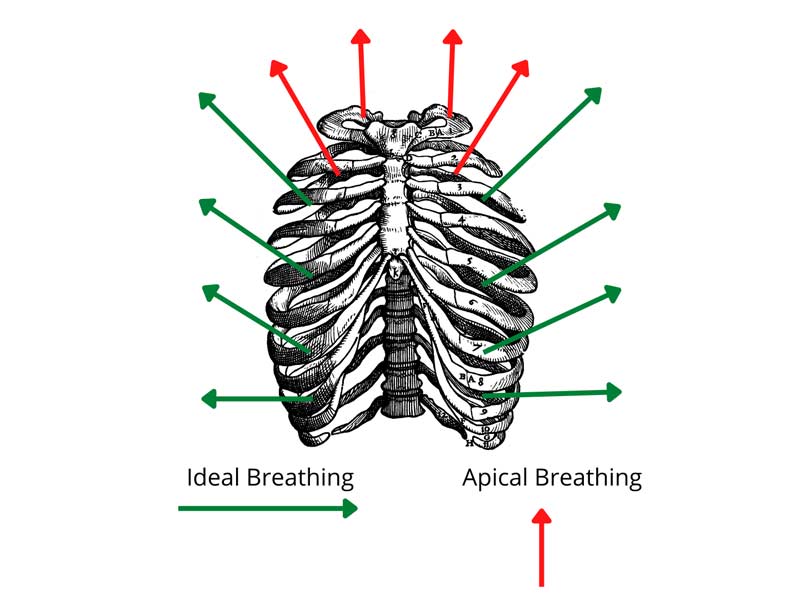
And the mechanics of an efficient breath — one that expands and compresses the entire ribcage with an active, mobile diaphragm — create fascial motion in most — if not all — of the body.
What I know for sure:
• Efficient diaphragmatic breathing creates a crucial wave-effect that mobilizes the gut (very much like this).
• Diaphragm inefficiency — stiffness and/or weakness — is associated with increased low back pain1, pelvic (and hip) alignment and mobility deficits2, and — as a result of that — any lower body dysfunction and pain.
• Inefficient breathing can strain the neck, by overusing lateral neck muscles to “apical [-only] breathe”, and is associated with cervical pain3.

If it can do all that…what else might breathing affect, mechanically and fascially?
Maybe everything?
Stay tuned for next week, when we dive deeper into the whole-body effects of efficient — and inefficient — breathing!
Cool Exercises I Like. Side Lunge Soleus Raise. The foot and lower leg is our connection to the ground. For athletic weight bearing — walking, hiking, running, jumping…and simply maintaining balance — we need a max-efficient foot, ankle and lower leg!
Here’s a real creative gem that works on strength, balance and agility and fascial mobilization of the lower leg into the trunk and pelvis, courtesy
What I like about it this bent-knee (soleus) raise:
• the staggered stance side lunge puts most of the weight into the bent ankle, maximizing ankle dorsiflexion
• performing a calf raise (ankle plantar flexion) in a sustained bent-knee position selectively strengthens the soleus muscle, which is a crucial lower leg, ankle and foot stabilizer.
• the focal loading of the forefoot mobilizes the first ray (ball of the foot and big toe) while working plantar foot and foot intrinsic stabilizers
• the wide side lunge position creates a frontal plane hip and pelvic fascial stretch that is accentuated with the dynamic foot-and-ankle motion.
• it’s simply a great (and fairly safe) way to work on balance!
Give it a try during a weight training or running warm-up!
Joe’s Articles. The Other Ankle Mobility. Ankle dorsiflexion gets a lot of attention in all athletics: it is crucial for fast running, peak strength and max agility.
Dorsiflexion is also key for injury prevention: decreasing knee strain, optimizing hip utilization, and decreasing compensatory low back strain.
But what about ankle plantarflexion? Often overlooked by athletes and sports med folks alike, plantar flexion is crucial for maximal hip-centric push-off, stability on uneven or technical terrain, and maintaining an athletic whole-foot landing.
But the coolest win-win? Mobilizing the ankle and foot into plantar flexion can also improve stubborn dorsiflexion!
A couple gems from an oldie on iRunFar.com,
Performance Mobility, Part 3: Foot And Ankle
Why Plantar Flexion Matters: Demanding terrain often causes stiff ankles, leading to compensatory patterns like hyper-supinated landings or “duck-waddle” shuffling, which reduce powerful push-off.
Consequences of Poor Plantar Flexion:
• Foot, ankle, and calf pain• Knee pain and stiffness (from increased knee flexion loading)
• Hip pain and stiffness (due to decreased hip extension)
• Low back pain
• Asymmetries can create stride imbalances and increase injury risk on the opposite side.
Assessment Test: Kneeling sit-back on heels (heels together and/or wearing shoes for added challenge). Goal is full, symmetrical plantar flexion with the tops of the feet, front of ankles, and shins flat on the floor.
Restorative Strategies:
Kneeling Sit-on-Heels: Static hold or gentle oscillations; modify with a pillow/towel under shins for severe stiffness or wear shoes for more stretch.
Shoe-enhanced weighted ankle plantarflexion. Sitting on the thicker heel of a running shoe enhances the posterior-to-anterior force on both the talocrural (ankle) and subtalar (talus-calcaneus) joints. Source: Author/iRunFar.com Kneeling Heel Pushes: Direct joint mobilization — place hand between ankle bone and heel, push downward toward the toes (10–20 oscillations per side). Can be done more aggressively if tolerated.

Self-mobilization of the both the talocrural and subtalar joints by hand. Pushing down with a focus on the ankle (malleolar) bones will emphasize talocrural; pushing directly on the heel, subtalar. Source: Author/iRunFar.com Important Note: Improving plantar flexion mobility also enhances dorsiflexion.
Takeaway: Regular foot/ankle mobility work is vital for maintaining strong, balanced running, especially with higher mileage and vertical gain.


{kind=link}
Victory Friday. Cross-Training Culprit in Chronic Pain? I had a fascinating session this week with a remote client dealing with foot pain.
Her favorite activity is running, but she incurred a foot strain in early January. It failed to improve with various mobility, strength and efficiency strategies. A subsequent MRI showed the following outcomes:
• an acute plantar fascial strain
• “tenosynovitis” — inflammation of the sheath around a tendon — of the medial ankle
• medial ankle joint (talus) stress
She had rested from running for over two months, and also had a PRP injection to the medial heel: the origin of the plantar fascia.
Since then:
• her foot pain is largely improved
however:
• she still gets “foot pain” — but it is no longer on the plantar surface. Rather, it is more forward and along the medial arch:

• other mobility and strength metrics are either normal or currently being addressed with home exercise. This includes lower leg fascial mobility and foot and calf strength.
• her biggest complaint: when she does comprehensive foot and calf strength, including single leg heel raises and eccentric loading…her foot pain gets significantly worse.
It feels fine during, but worsens — feeling tight and achy — a couple hours after strength work.
Lastly, I asked about activity level.
She had not run in two months. But what she was doing: the elliptical trainer.
And a lot of it. “60-90 minutes a day” of elliptical exercise, seven days a week.
🚨🚩
This is cause for concern, and not just for her mental health (who can endure that much elliptical once, let alone every day?)
If we put it together:
• medial ankle and arch pain
• an imaging finding of medial ankle tenosynovitis
• latent pain after plantarflexion strength
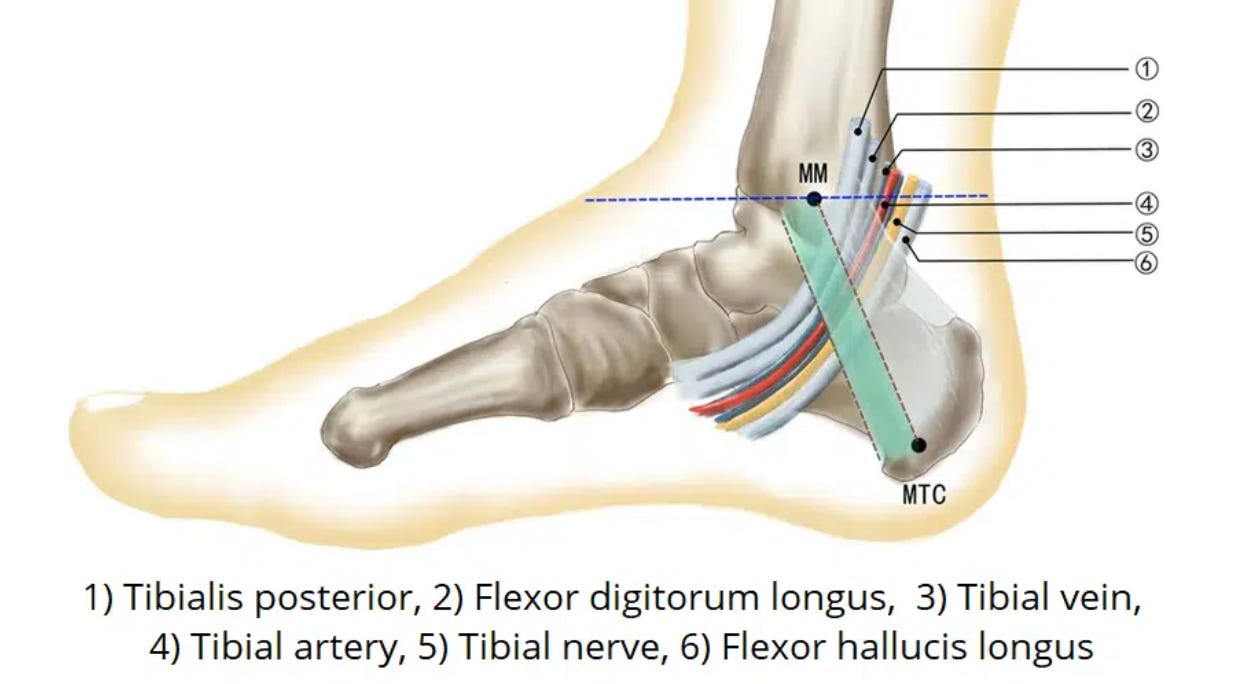
I suspected her remaining pain was not the plantar fascia, but the tendons of the medial shin and ankle:
And what did the elliptical have to do with it?
When you “ride” an elliptical trainer, the plantarflexors are pushing into the foot platform, non-stop:
This means those shin and ankle muscles and tendons are under constant tension for 60 to 90 minutes!

And even though she didn’t feel significant pain during elliptical training4, I strongly suspected that this prolonged load was overloading those foot and ankle structures, preventing full healing, and causing pain with the higher-intensity eccentric work.
Based on the information and this theory, I:
• recommended she stop all elliptical training for two weeks — and do no weightbearing cross training for at least 2-3 days
• try the eccentric foot and calf strength in 2-3 days and gauge soreness after this rest.
The Early Returns. Since doing so, she reports:
• marked reduction in foot symptoms during the day
• decreased latent soreness after strength work
Going Forward. Rather than elliptical, she will begin uphill treadmill hiking as a non-running aerobic alternative.
Unlike elliptical, hiking is a natural movement that involves a normal contract-relax, loading and unloading pattern:
• landing and pushing off with the foot and lower leg (loading)
• a swing phase with forward stepping (unloading)
I anticipate this will feel better, as well, and — very soon — she’ll be back to running!
Takeaways. Always Survey Clients for Provocative Activity! I always say:
The cruelest irony for injured runners:
grinding through high volumes of miserable cross-training to compensate for not being able to run — yet that very cross-training often prolongs the injury and delays their return to running!
Assess all physical activity for potential tissue overload, especially in cases where the “other bases are covered”, including:
• rest
• mobility and strength exercise
• regenerative treatments
Issue 137 is a wrap!
Help people move, function and feel better: please share this publication!
Thanks for reading, and have a great weekend,

Issue 74: Low Back Pain & Impaired Diaphragm Function. A study of elite weightlifters found that those with chronic low back pain exhibited significantly reduced diaphragm function — lower thickness, excursion (mobility), and maximal inspiratory pressure —compared to pain-free lifters. Lower diaphragmatic pressure also correlated with poorer snatch and clean & jerk performance. The authors suggest diaphragm strengthening may improve both sports performance and low back pain management.
Issue 40. “Hips In Captivity”: Diaphragm Dysfunctions Hindering Hips. Treating diaphragm restrictions in two young runners (male distance, female sprinter) with hip pain and pelvic/hip dysfunction resolved ~75% of mobility and alignment issues before any direct hip/pelvic work. This underscores the diaphragm’s key role—via fascial connections—in pelvic/hip alignment. Recommend assessing thoracic mobility and diaphragm function in all lower-quarter clients.
Issue 17: Gregg’s Gems. Effect of diaphragmatic breathing, respiratory muscle stretch gymnastics and conventional physiotherapy on chest expansion, pulmonary function and pain in patients with mechanical neck pain: A single group pre pretest-posttest quasi-experimental pilot study. A study on patients with neck pain found that daily diaphragmatic breathing (only 10 breaths) combined with respiratory muscle stretch gymnastics significantly improved chest expansion, reduced pain and dramatically lowered neck disability scores. This adds support for addressing thoracic mobility and breathing mechanics in cervical care, likely through fascial connections.